Laboratory Diagnosis of IPA
Dr Ariya Chindamporn
Associate Professor, Department of Microbiology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Like other fungal infections, direct examination, culture and non–culture-based methods including histopathology, serology and polymerase chain reaction (PCR) are the general protocols for laboratory diagnosis of aspergillosis. The recommended specimens are sputum, bronchoalveolar lavage (BAL), blood and tissue from biopsy.
Direct examination of any specimen by potassium hydroxide (KOH) preparation (Figure) and Gram stain are the priority for prompt information. However considering its natural distribution being practically everywhere, the presence of septate hyphae of Aspergillus fumigatus, is not significant for diagnosis. To obtain a strong documentation of infection, thorough investigation by collecting multiple specimens is recommended to increase the yield of positive cultures from multiple samples, especially from BAL.
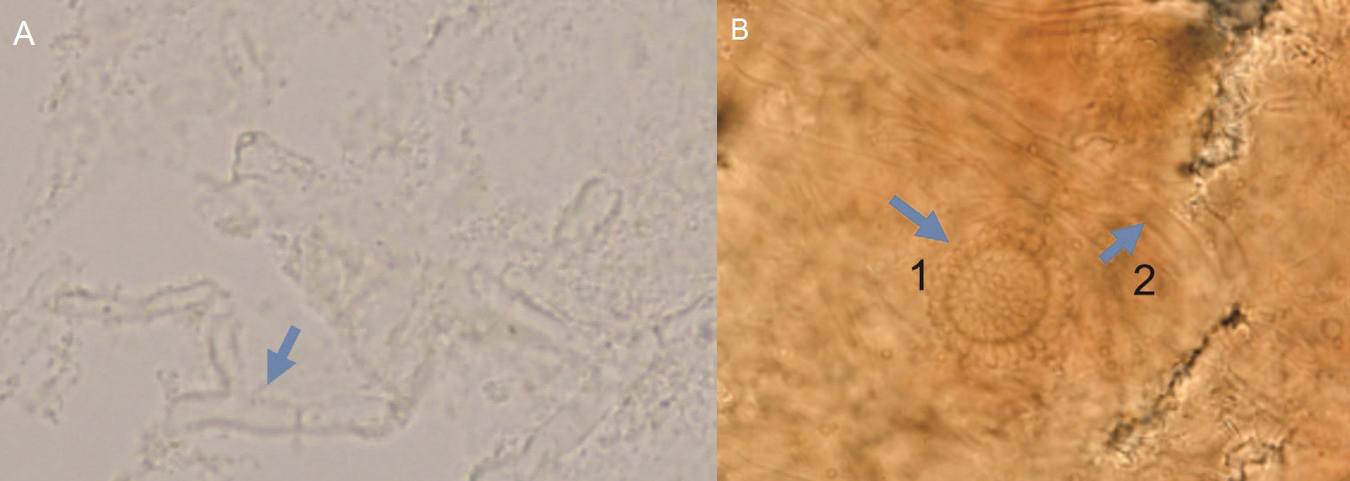
Figure. Potassium hydroxide (KOH)-preparation of bronchoalveolar lavage sample showing (A) septate hyphae, and (B) phialide from the top view (1) and septate hyphae (2) (x400)
{kind=link}
Recently, aspergillosis has been found in both immunocompromised and immunocompetent hosts. Based on the 2016 European Respiratory Society (ERS) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the management of chronic pulmonary aspergillosis,1 the key laboratory tests for respiratory specimens are direct examination, histopathology and fungal culture, with the last being the best diagnostic procedure. Furthermore, BAL specimen is recommended for patients with cavity or nodular pulmonary infiltration. PCR is another choice for laboratory diagnosis.
Galactomannan assay from paired samples of BAL or serum is a non–culture-based diagnostic test. The sensitivity and specificity of galactomannan testing in BAL sample is 77.2% and 77.0%, respectively, with the cut-off level of 0.4; and 85.7% and 76.3%, respectively, with cut-off level of >0.5. For serum galactomannan testing for the diagnosis of chronic pulmonary aspergillosis, the sensitivity and specificity rates are 66.7% and 63.5%, respectively (cut off level 0.7). Aside from the detection of galactomannan from the fungal cell wall, (1-3)-β-D-glucan is another component that can be examined as well. Even though positive results from these two assays are not definite indications of the fungus, negative results from these tests can provide strong evidence that the sample/specimen does not have non-septate hyphae.
Reference:
- Denning DW, et al. Eur Respir J 2016:47:45-68.